Are psychotic experiences something that should simply be suppressed? These experiences cause so many problems, it may seem that the answer should always be yes!
But there’s a paradox when we try hard to get rid of psychotic experiences. Our efforts to do so can quickly make the problem worse!
At its simplest level, we see the basis for this when we try too hard to get rid of a thought. For example if you focus too much on not thinking about elephants, they will be on your mind all day. If you focus on not having the thought that you might have germs on your hand, you might spend all day washing your hands to make sure there is no basis for the thought.
And if you are very sure you shouldn’t be having a thought, it might start to seem that the thought is coming from somewhere else, like a brain implant or a demon or telepathy from someone you don’t like. Now the battle is really on! But the prognosis for winning this battle is not good. Efforts to get rid of what now seem like voices etc. just make them seem more important and more compelling. Things can rapidly spin out of control, and go to some really dark places, which often just convinces everyone involved that doubling down on attempts at suppression is the way to go!
Fortunately, there is a better way. Paradoxically, it involves accepting even the “crazy” thoughts or voices that seemed to be causing so much trouble, but in away that avoids making too much of them.
Our brains are weird, our minds are weird, and that’s OK. We can learn to help people not make too much of the weirdness, and to identify what helps them move on and make a life they value, and to connect with the people and activities they love.
Finding the common humanity within the sometimes freaky experiences that get called psychosis is a key part of the CBT for psychosis approach called “normalizing.” It can help a lot in getting people to change their relationship with tricky experiences, rather than seeing those experiences as pathology that requires suppression and elimination.
If you would like a better idea of what normalizing is, check out this video:
For those who want to learn more about how CBT and a few other therapy options can be helpful for psychosis, or what gets called that, there is a series of 5 seminars that I am offering over the next few months. Attending one or more of these seminars could be a very affordable way to grow your competence in a psychological approach for psychosis – and you can save by accessing Early Bird pricing that only lasts through 4/5/24!
Each seminar will be 4 hours long, and will provide time for questions, discussion, and practice. Continuing education credits will be available for most US professionals. Each seminar will be recorded, and those who register will have access to the recording. CE credit however will only be available to those who attend the seminar live (on Zoom, or in person in Eugene OR) for the entire seminar.
The seminars are:
Date: 3/29/24 – Essential Elements of CBT for Psychosis: Engagement Style, Normalizing, & Developing a Formulation
Date: 5/10/24 – Paranoia and Troublesome Beliefs: A CBT Approach
Date: 6/21/24 – Voices, Visions, and Other Altered Perceptions: Changing Outcomes with CBT
Date: 7/19/24 – Trauma, Dissociation, and Psychosis: CBT and Other Approaches to Understanding and Recovery
Date: 8/16/24 – Addressing Cultural and Spiritual Issues Within Treatment for Psychosis
The most affordable option is to register for all 5 seminars as a bundle (only 59.99 per seminar if you register by 4/5/24) but you can also register for seminars individually.
When people report the extreme beliefs that are often labeled “delusions,” it can be difficult to know how to make sense of what is going on and what might be helpful. That’s why I took the time to review a new book on the subject, “Decoding Delusions: A Clinician’s Guide to Working with Delusions and Other Extreme Beliefs,” edited by Kate V. Hardy and Douglas Turkington.
What follows is a draft version of the review, but if you are one of the first 50 people to click on this link, you can see the final version that is now published online in the journal ‘Psychosis.”
Delusions are commonly understood within a medical model, but this book challenges that, starting with the title! That is, the assertion that delusions might be “decoded” implies that with some effort we might come to understand them, a notion that is in sharp contrast to the prevailing belief that delusions are just the meaningless product of a brain that has become ill.
We tend to call a person’s beliefs “delusions” when we can’t come up with a better understanding of why the person believes them. This can provide some relief for us: if the strange belief is simply caused by an illness, then we don’t have to wonder any more about any meaning we might be missing or how the belief might be an understandable result of the person’s life experience. Unfortunately, while this may make us feel better, it risks trapping the person with the strange belief in a lifetime of confusion and disconnection, where people around them give up trying to understand them and where they also come to believe that it is pointless to try to understand themselves.
In contrast, “Decoding Delusions” offers multiple perspectives on both the possible sources and meaning of these beliefs and on how to help people understand themselves and how to experiment with shifting views in ways that can reduce distress.
The chapters of this edited collection offer varying points of view, including views drawn from lived experience, from contrasting theoretical perspectives, and from people working in different settings and with different cultural groups. And to facilitate working with those different cultural groups, it includes guidance in thinking about extreme beliefs through a cultural lens.
One angle well covered in this volume is the possibility of delusions having their source in traumatic experience. The impact of understanding them this way can be profound, as evidenced by this exchange reported in one of the chapters:
“’I am going to tell you that there is absolutely nothing wrong with you.” Quite taken aback, I said, “But I’ve been told I have schizophrenia; I have been told that I will never recover.” He said, “I know what you have been told, but I am telling you there is nothing wrong with you whatsoever. This is normal, it’s not illness. In the context of your life, this is normal.’”
Of course, letting someone know that their way of thinking may be an understandable reaction to their life events is just a beginning; the bigger challenge is to help them modify those reactions and to find a new perspective on the world. This opens the door not only to reducing distress but also creates opportunities for people to recover and to regain control of their life. Here, the book also has a lot to offer: it describes many cognitive behavioral approaches to change but also other promising approaches drawn from sources such as psychodynamic and compassion focused therapy.
Human beliefs come in many forms and varieties, including those which are called delusions. The book explores ways of understanding and working with many forms of delusional thinking, including persecutory paranoia, delusional jealousy, erotomania, Capgras syndrome, and delusions of thought possession, and it compares beliefs that qualify as delusions held by individuals with the often equally wild conspiracy theories that are of increasing popularity within many subcultures.
As a bonus, the book includes links to a series of video examples illustrating effective therapy approaches for people who seem to have delusions (along with a couple of illustrations of approaches that are likely to be ineffective or to backfire.) People with delusions often seem stuck in unhelpful beliefs, but the mental health field has also been stuck in unhelpful beliefs about such delusions. The contributors to this book deserve credit for guiding us into taking a fresh look at the evidence and considering more helpful perspectives.
One other resource of note on alternative ways of understanding and working with “delusions” is this video presentation by Rufus May – a psychologist who was once hospitalized due to his own extremely paranoid beliefs!
I often hear from family & friends of people with psychosis that they want to be helpful but don’t know how. So I put together a list of resources that might provide some guidance.
Or parents who are skeptical of conventional drug-based treatments for children struggling with mental health issues and who are looking for alternatives may be more interested in Mad in America’s online parent support groups.
Some of these resources, in particular NAMI, may be at times overly invested in describing psychosis as definitely an “illness” rather than as a possibly understandable reaction to difficult or confusing life experiences. But there’s a lot that can be helpful in these resources, despite their imperfections.
Sometimes the emphasis on “blaming the illness” comes out of a reluctance to say anything that might lead family or friends to blame themselves in any way for how their loved one became lost and confused. This has led leading organizations to promote statements like “Psychosis is nobody’s fault. People do not cause it.” Unfortunately, as I have written about before, this leads to a denial of how trauma and in particular interpersonal trauma is often a big cause of psychosis, and also to ignoring how other kinds of stressful and confusing life events can play a role.
My perspective is that rather than teach family members to “blame the illness” as a way of avoiding getting caught up in self blame, we can instead guide them in finding a middle way. That is, we can acknowledge that life is tricky and confusing, our brains are tricky and confusing, and because of this we family members may not always have been helpful to those we love and care about, and sometimes we may have been clearly unhelpful or hurtful in ways that may have contributed to the psychosis. But this does not have to mean getting caught up in blaming ourselves; we can instead shift our focus to learning what we can do now to be part of the solution. In other words, we can model accepting ourselves as imperfect and sometimes confused and confusing people who nevertheless can love and value both ourselves and others in the present- the same sorts of skills that will be so useful to our loved ones in their own journey toward recovery.
Back in 2015 Paris Williams wrote a 3 part series on Madness and the Family, see Part 1, Part 2, and Part 3 that explores some of the complexities around psychosis and families. Or you might also appreciate hearing a 45 minute talk he gave on the same subject
While it’s still common for people to be told that psychosis is a brain disorder that was not caused by anything anyone did to them, there is now an extensive body of research that indicates that traumatic experience can be a cause of psychosis, and the link between having multiple types of trauma and later psychosis is close to the strength of the link between smoking and lung cancer.
But what is the nature of the connection between trauma and psychosis? One factor that seems to play a role is that of dissociation, which is something we all do at times but which is often very strongly triggered by trauma.
To help professionals understand and work with this issue, I offered a free one hour webinar “Trauma, Dissociative Splits, and Psychosis: Approaches to Healing” on Friday April 21st – the recording is now available, see below. (This event was hosted by APA Division 18 Community and State Hospitals Section.)
Here’s the description for it:
“Dissociation is a factor that can mediate the relationship between adverse life experiences and psychosis. This webinar explores how methods drawn from diverse sources like evidence-based practice (CBT) and peer support/lived experience (Hearing Voices Movement) can help people regain perspective and personal power. Discussion regarding the utilization of effective psychosocial interventions and supports to promote healing and quality of life will be conducted.”
Learning Objectives:
Explain how dissociation as a trauma response can create risk for psychosis.
Identify and describe at least 2 therapeutic interventions for dissociation that also reduce distress related to psychotic symptoms.
Describe at least 2 individual factors to consider when selecting and adapting treatment for trauma and psychosis.
There are also recordings of a couple of earlier webinars that you can view:
Trauma and Psychosis: Exploring the Intersection
Moving from Trauma and Psychosis to a Recovery Story
Traditionally, psychiatry has taken the position that “getting out of your mind” is a bad thing: they have made “normality” in thinking the standard for health, with experiences going outside of that being viewed as pathology.
But more recently, there has been an interest in using psychedelic drugs within psychiatric practice. That’s because traditional approaches to psychiatric practice haven’t helped very much, and some studies show that shaking things up with psychedelics can at least sometimes break people out of unhelpful patterns and set them on a better path.
This however raises a lot of questions. For example,
If going somewhat out of one’s mind on psychedelics can be a good thing, then maybe other experiences of going out of one’s mind also have possible value which psychiatry has been ignoring?
On the other hand, if going out of one’s mind is often related to problems, is it possible that attempts to use psychedelics in treatment will lead to many people getting into increased difficulties? And then when/if this does happen, will psychiatry blame this on an “underlying illness” much as it often does when. say, antidepressants trigger a manic episode?
Is it possible that our entire culture needs a better understanding of ecstatic mental states that take one outside one’s usual state of mind, before we have any chance of handling such issues?
Jules Evans is a philosopher whose perspective has been shaped by experiences that included early use of psychedelics, including both apparently helpful experiences as well as a bad trip that caused problems that lasted for years, and an ecstatic near death experience. He argues that our society needs to become more literate about ecstatic experiences of all kinds, in a way that appreciates both their gifts and their dangers.
Jules is the author and/or editor of some interesting books, including
and
Perhaps because his own experiences have been so varied – ranging from extremely helpful to extremely not – I think Jules does better than most in addressing this topic in a balanced way.
Psychiatrists commonly pathologize extreme and ecstatic experiences, while some who oppose psychiatry may seem to romanticize them – but what we really need is a deep understanding of the multiple sides of such experiences. Kind of like with fire – fire is both great and very helpful, and quite terrible, and we do best with it when we are aware of this duality.
If you would like to learn more about this point of view, I encourage you to check out this recording of the ISPS-US webinar “The Mysticism / Psychosis Continuum, with Jules Evans,” of a talk given on 3/17/23. Note that the talk itself is about an hour, followed by an hour of question and answer.
I recently wrote a book review for “Relating to voices using compassion focused therapy: a self help companion” by Charlie Heriot-Maitland and Eleanor Longden. Here’s what I said:
“A friend of mine who eventually recovered after spending many years in hospitals being treated for “schizophrenia” complained to me that all the professionals who treated him never mentioned “love” or anything like it – yet that was the essential ingredient he required to heal.
“Professionals have often been taught that to be scientific, they should avoid the “warm and fuzzy” while focusing instead on suppressing or eliminating “psychopathology”. But compassion focused therapy, on which this book is based, takes the opposite stance. It argues that while our brains have evolved to be tricky, and prone to getting stuck in destructive “loops” and inner conflicts, we also have an evolved capacity for compassion, and that the key to healing is learning to use compassion to reconcile with, rather than suppress, the parts of our minds that disturb us.
“This book makes this compassion focused approach accessible to voice hearers. The kindness and humanity of its coauthors (one of whom is herself a voice hearer) are a consistent presence as the reader is thoughtfully guided through possible steps toward changing relationships with voices.
“To begin, voice hearing is normalized as a normal human experience, and reasons to take a compassion focused approach are introduced. Issues of being safe and feeling safe (not always the same thing!) are discussed, and ways to access and/or develop a “compassionate self” are introduced. The next step is learning how to explore one’s conflicting emotions or “emotional selves” from the perspective of the compassionate self. This is good preparation for relating to voices, since emotional conflicts are usually less tricky than are conflicts with voices. Then comes work on developing a compassionate understanding of the voices and of their activity. By considering early experiences and key fears, voice hearers learn to discern how even voices that appear wildly destructive may have a protective intent. Finally, equipped with that perspective, ways of compassionately and wisely relating with the voices and with the emotion behind them are introduced.
“To support this journey, a variety of methods are employed. There are “check-in” boxes that encourage readers to notice how they are responding to what is being introduced, and “practical boxes” that lead the reader in exercises to practice new approaches. There is also a companion website to the book, relatingtovoices.com, which contains audio and print versions of the exercises, along with links to videos and other resources.
“While written as a self-help book, it will also be useful to professionals and to family members who want to increase their ability to support someone in using this approach, even those who may not themselves be inclined to read books.
“One of the persisting myths about mental functioning, which is especially destructive to voice hearers, is the notion that experiences of something hostile or disruptive within our mind is likely the sign of something wrong with our brains. This creates excess dependence on drugs and on a continued battle with whatever is disruptive, in a way that too often inflames into what one of the authors, Eleanor Longden, has referred to as a “psychic civil war”. By instead framing contrary emotions and emotional systems, as well as voices, as all deriving from evolved systems that are trying to help us (even as they may go overboard with that), compassion focused therapy and this book in particular point in a much more hopeful direction, creating possibilities for peace, healing, and the kind of true mental health that has its origin in our hearts.”
If you’ve ever been tempted to think of hearing voices and of “psychosis” as just something medically going wrong with one’s brain, I can think of nothing better than a recently released video to convince you otherwise!
In an awesome performance linked to below, Ren dramatizes a battle between himself and an apparently evil voice that seems bent on tearing him down. It progresses into an amazing intensity, then a resolution or transcendence of the battle that may stun you with its humanity.
Anyway, check it out. Note that the first comment listed on YouTube contains the full lyrics.
We sometimes like to think that our minds work all as one whole – but parts of us may not agree with that!
Even in everyday experience, we may notice conflicts within ourselves. Part of us wants to keep working, while another part thinks we have done enough for today. Part of us wants to stay in the relationship, while some other parts have had enough. Part of us wants to stay on the diet, while another part is eyeing the chocolate cake.
But what is the relationship between these everyday “parts” and the experiences that get called psychosis? And how might treatment for psychosis be different if we better appreciated the role of parts and worked explicitly with them?
Those are questions I addressed in a talk I gave at the 2022 ISPS-US Conference, the recording of which is below. Here’s the title and description for the talk:
Integrating CBT for Psychosis with Parts Work and Internal Family Systems
Cognitive Behavioral Therapy (CBT) for Psychosis has proven its effectiveness in over 50 research studies, and its methods are relatively straightforward. But the human mind and experience is full of complexities, contradictions, polarities, and multiplicities: is it possible that CBT is simply “too straightforward” to address all of this?
Meanwhile, therapies have been developed that explore the many possible “parts” of people and the relationship between those parts: for example, Internal Family Systems (IFS). These approaches provide a coherent way to dive below the surface and to work with internal complexity. However, their application to the field of psychosis is still new, is not well researched, and it is often unclear how they might best be applied in specific situations or to address the various dimensions of psychosis.
This presentation explores the possibility of integrating CBT with deeper approaches such as IFS that acknowledge the existence of distinct and partially autonomous parts within people, and complex internal relationships between parts. Ways of resolving the conflicts and contradictions between CBT and IFS are explored, and possible areas of synergy are identified. The aim is to show how therapists might draw from the best of both approaches to provide people experiencing psychosis or extreme states better opportunities for healing. People have both surfaces and depths: isn’t it possible that therapy can work with both, in an integrated way?
Support in returning to school or employment after any kind of mental health challenge can be a key piece in helping people regain control of their life and avoiding a lifetime of disability, inactivity, and stigma.
And such support can be very effective: over 2 dozen studies show that most people even with diagnoses like “schizophrenia” who want to work can succeed in competitive employment.
But people challenged by the confusing and/or extreme experiences commonly called “psychosis” often don’t get such assistance, sometimes because helpers may not understand the difficulties being encountered or know what kind of support might be useful.
To help remedy that, I’ve put together a couple of presentations that explore perspectives and strategies borrowed from Cognitive Behavioral Therapy (CBT) for psychosis and from the Hearing Voices Movement, approaches that support workers, friends, and family members can use to help people achieve their educational and employment goals. I hope you check them out, and let me know what you think!
PART 1:
PART 2:
I also put together a short list of resources related to what I talked about, that is available here.
When deciding how to organize treatment for “psychosis” we face a crucial question. Should we defer to mainstream views and assume that “psychotic” experiences must be part of an illness? Or should we stay open to the possibility that the confusion and distress we witness may be resulting, not from something wrong with the brain, but from people experimenting with sometimes extreme strategies to cope with difficulties in their lives? And that possibly the confusion and distress we see is created when people experiment with strategies that may backfire in ways they do not understand at the time?
In this post I will be making the case that psychosis is often more of the latter. To illustrate, I will focus specifically on what can happen when people experiment with the competing strategies of skepticism and faith.
Being skeptical, or alternatively having faith, are both examples of strategies people use effectively at different points in daily life. But like a lot of strategies, they can also backfire.
Skepticism involves being able to encounter evidence for something, yet not believe it. So we might read about something in the newspaper, or hear about it from others, or even see something with our own eyes, but yet not believe it is real or at least not be sure it is real.
This is a very helpful strategy when we are exposed to misinformation or partial information, or to sensory illusions or dreams, etc. Of course, it’s not so helpful at many other times, such as when someone is telling us the truth, and we fail to believe them or to act on it in time. Then skepticism backfires.
Faith it seems is an opposite strategy. Faith involves our ability to believe something in the absence of evidence or even when exposed to evidence that the belief is wrong. So we might hold onto a belief that our partner is loyal to us even when confronted by evidence that suggests they are cheating, or hold onto a belief that our business will succeed even when the initial financial reports are dismal.
This is a very helpful strategy say when our partner really is loyal and when it only appeared that they were cheating, or when our business idea is sound but is just slow in becoming profitable. It isn’t so helpful when our partner really is cheating, or when our business idea is hopelessly flawed.
What I’m proposing is that there’s always a tension in our lives between these two strategies, which are designed to meet opposing yet equally valid needs.
One the one hand, we have a need to need to be able to question our beliefs and to be open to disconfirming evidence, so we can avoid continuing to believe what is not true.
On the opposite side, we often have a need to hold on to beliefs in things that are true—even in the face of apparently disconfirming evidence.
But because they are opposites, a dilemma arises. How are we to know when and where to focus on having faith, and when and where to instead practice skepticism? Certainly there are “sources” we might turn to which would tell us, or habits we could follow, but when and where should we have faith in those sources and habits, and when and where should we be skeptical?
One proposed solution to this dilemma might be to define mental health as having just a moderate amount of each: a moderate amount of trust or faith in the media and in other people and in our senses, combined with a moderate amount of skepticism about each of those things.
But I would argue that it’s more complex. Some situations call for more extreme or radical forms of faith, and/or of skepticism. We need to be more extreme to find the truth in some situations that are tricky or where a lot of deceitful evidence may be present. Such situations may exist either for some natural reason, or due to the functioning of a misguided culture or a conspiracy, or all of the above.
For example, imagine the situation of a person who is being told by everyone they know, and by the media, and by mental health professionals, that their depression is due to a lack of serotonin in their brain. To handle that situation well, this person might have to have very strong faith in their intuition that the depression is more a reaction to life events and psychological processes, and to maintain a very firm skepticism about all the social pressure to believe in the chemical story.
One thing I hope you notice in the above example is that there is an interplay between faith and skepticism. To strongly hold faith in some belief, we need to develop strong skepticism about the evidence that contradicts the belief. At the same time, to be strongly skeptical of some evidence, we need strong faith or trust that we can be OK while disregarding the evidence. That gets harder to do when the stakes get higher. An example illustrating such a difficulty was a study where many people would refuse to drink from a beverage labeled cyanide, even after they had been told by the researchers that the label had been applied just to test their reaction to it. It seems they weren’t quite able to doubt or be skeptical about the label when their life was at risk if they were wrong!
As we proceed in life, we are constantly comparing evidence from our own experience with opinions and evidence offered by others in our social world, and then developing ideas about what to believe in and what to be skeptical about. At times, this process can lead us down an unhelpful path, where we get stuck in beliefs in things that aren’t true and being skeptical about things that are true. To get in touch with what is really going on we might need to radically question what we had been believing, and to develop some new belief and then hold onto it even in the face of pressure inside ourselves and from others to revert to a prior point of view. The ability to make such changes in our understanding, or paradigm shifts, could be framed as a kind of superpower. It’s an ability, a feature of our minds, not a defect.
But these same abilities can also lead us into a lot of trouble. They must be used with great discretion to avoid catastrophe. Without that, we might be doubting everything and lost in uncertainty when we might better be following previous ways of thinking, and we might be holding firmly onto radically new conclusions that we would better off questioning.
One curious fact is that psychosis first occurs disproportionately in people who are in their late teens or early adulthood. A possible explanation for this is that this is because the ability to have radical skepticism and radical doubt first develops at this time of life. Just as many types of young mammals go out seeking their own territory at a certain age, humans at a certain developmental stage develop an ability to have an independent point of view, an ability to possibly see things very differently than how everyone else is seeing things.
But a problem can be that these abilities typically emerge when the person does not yet have the judgment to use them wisely. Traditional tales like The Sorcerer’s Apprentice illustrate this kind of situation, where a useful power becomes a big problem when someone does not know how to use it correctly or to stop it.
In thinking about this I’m drawing from my own journey. As a child, I was abused at home and extensively bullied at school, plus I was gay and my community didn’t like that. This led me to have a sense that I was an inferior person, and others around me seemed happy to confirm that.
But there was still part of me that wanted to believe I was OK, or even great! To shift to seeing things that way I had to deeply question a great deal of what I had previously experienced and learned from my interactions with others. So questioning is what I did; but once I started questioning so much of what I had learned and of what my identity had been, it wasn’t obvious to me where I should stop.
We are often told that schizophrenia is an illness where people lose their sense of self, and their sense of a stable world. But I don’t think we talk enough about how such a breakdown can be a strategy like it was for me, an attempt to break free of a sense of self and world that feels or perhaps is inadequate.
One question worth asking is, what happens to our mind when we radically question everything?
It seems we lose our ground, we lose our stability. We can’t trust the media, we can’t trust other people, we can’t trust our memories or our senses. Everything is in doubt.
Where are we then?
A sort of nowhere place, in a great void or question mark or cloud of unknowing. Tumbling in an abyss.
And in a sense, we also seem to be everywhere, because now anything seems possible, anything might be what is “really happening.” Including anything threatening.
Bertrand Russell stated that “Skepticism, while logically impeccable, is psychologically impossible, and there is an element of frivolous insincerity in any philosophy which pretends to accept it.”
Because the loss of a definite world and of an intersubjective sense of reality due to extreme skepticism can be so intolerable or impossible, it’s a common reaction to then go to the opposite extreme, where we grasp at something to believe to give us stability.
But then the danger is that we might grab too firmly, and have faith in the wrong things.
We know that in addition to lacking a sense of self and world, people diagnosed with psychotic disorders often have excessively firm ideas about themselves and the world.
Paul Lysaker once asked someone with a fixed belief why he held onto it so strongly. He answered, “it keeps the vacuum from sucking away my brain.” It seems he was afraid of that emptiness we can encounter when we question everything.
Experimenting with radical forms of skepticism and faith can also lead to inner divisions, conflict, and confusion. People might become skeptical of their own thoughts for example, and start wondering, are those thoughts being put there by someone else? Or skepticism might lead to such a lack of clarity about what to do that when voices emerge that do propose a clear direction, the person might put radical faith in them and act on them without further consideration.
But now let’s consider how the mainstream mental health system typically interacts with people who are struggling with these dynamics.
It essentially tells people to be radically skeptical of their own mind and subjective reality, of their own process of skepticism and faith, and to frame what is unique in their point of view as just “mental illness.” They are pushed to use drugs to reduce the intensity of their independent thinking. And they are asked to radically trust the professionals and others around them to have the correct point of view, even when that strongly contradicts the person’s own perceptions.
This isn’t balanced. It asks people to be mentally passive and to give up on the possibility that their own mental process might be headed toward important truths even when those thoughts and perceptions contradict the viewpoint of others around them. There’s something healthy about resisting the demand for such a surrender of any faith in oneself!
The emerging dialogical approach, fortunately, is quite different. It doesn’t ask people to have extreme skepticism toward their own unique point of view, and such faith in the view of others. Instead it embraces uncertainty and polyphony, which includes the notion that the truth is usually too complex to be held entirely in any one way of viewing it. So there is skepticism about the notion that any person or voice or point of view has a lock on the truth, while also faith that each voice or way of looking at things has some value.
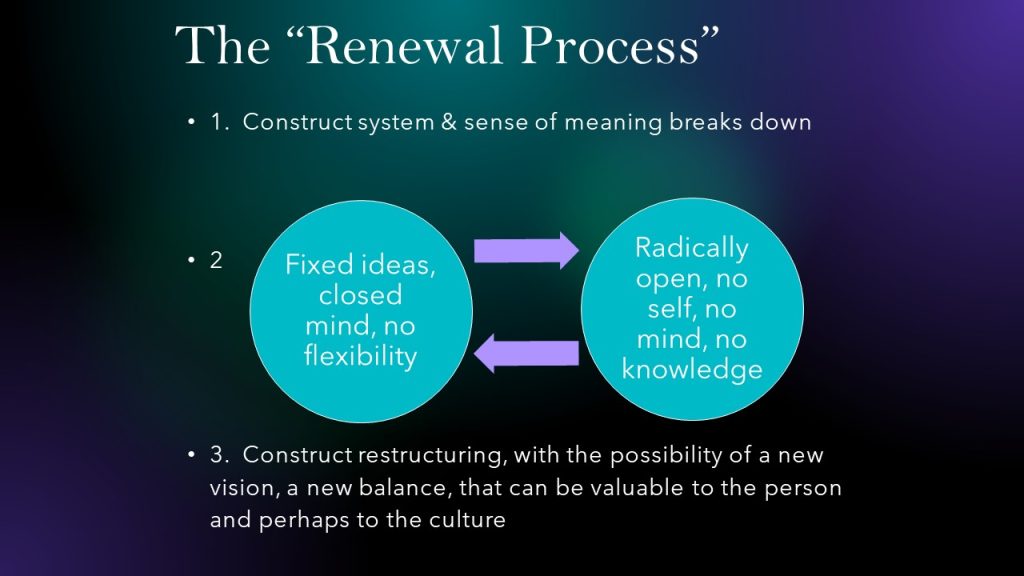
I believe that when mental health professionals take a more balanced or dialogical approach, then people they are attempting to help have a better chance to find a new balance for themselves. With such support, the whole process of going mad has a better chance of becoming something more like a renewal process, or a process of revolution that has a chance of leading to something better, as illustrated below:
We should not be surprised when sometimes young people lose faith in the views of the world they have grown up with and inherited, and with the sense of meaning that they have developed up until that point. There may be something in those views or that sense of meaning that they just can’t stomach anymore, or they may start sensing and believing in the existence of things others don’t acknowledge. They leave a shared intersubjective world, or simply don’t believe in it anymore.
They then enter a middle stage, where they may be exploring extremes and often bouncing between opposite strategies. Radical skepticism may have them in some way lacking a sense of self or a coherent map of the world and, alternatively, radical faith may have them hanging rigidly onto a fixed sense of self and of the world even when that doesn’t work well for them.
At this stage, they may seem lost, and “mentally ill,” and those around them may feel their only hope is to convince the person that they are ill and that they should suppress their own views and surrender to the viewpoint of others. But if this happens, the renewal process is aborted, and the person is left with a sense of having a defective mind.
The saying “when you are going through hell, keep going!” applies here. When we interrupt a person’s radical experimentation and attempt to reimpose an old order, or to have the person frame their own process of breaking away from that order as nothing but illness, people end up in a disabled state. Professionals and family members might hope the person could just go back to being like they were before, but there may be no going back. Instead, the effort to stop the process leaves the person stuck in something like a calm place—in hell.
I suspect one of the reasons why psychosis may then so often “reoccur” is that being stuck in this way eventually becomes intolerable, and the person’s mind again makes a break for freedom—resulting in more chaos.
What is important though is that there is another option. With the right kind of encouragement and support, a person can keep the process of experimentation going, and then often work through their confusion and find a new balance, at a third stage, a stage of return.
In this new balance, they retain their new ability to be radically skeptical of established views and to have radical faith in their own ideas, but they also become able to use some discernment about when and where to invoke these strategies or superpowers. They learn to balance the possible value of breaking away from established views, with the possible value of going along with them and thinking more conventionally. One way of putting this is that they learn to bring their “mad” views into dialogue with more conventional views, a dialogue in which those mad views are still valued, but not overvalued.
This is the return stage of the hero’s journey, where the person comes back to their community typically bearing gifts that resulted from the journey. These gifts can be new understandings and views that may benefit themselves and possibly that can be shared with and revitalize their community.
And our society does very much need to be revitalized! Sadly, what passes for sanity in our society is often not very sane. I’m always reminding people of what my friend David Oaks says, that “normal people are destroying the planet.” And while the process of experimenting with radically different views is dangerous, and often leads to distress and unhelpful views and confusion, it is a critically important process for “questioning normality” that we suppress at our peril.
The better option is to recognize the value of the process, but also find ways to avoid its pitfalls, by keeping the experimentation and the dialogue going till we find something better. One thing that would facilitate this would be creating widespread recognition that it is a process of experimentation, and not an “illness” that needs to be eliminated.
****
Note: This post is based on a talk given at the ISPS International Conference in Perugia earlier this month. ISPS conferences explore new ways of understanding and approaching experiences seen as “psychosis.” The next ISPS-US conference, November 4-6, 2022, will be a hybrid, with options to attend online or in person in Sacramento CA. Discounts for people with lived experience, and some scholarships, are available. Early Bird prices end 10/4/22. For more information or to register, go to this link.
This 6 hour course presents evidence based, practical and humanistic ways to help people recover. For more information or to register, go to this link.
Working with Trauma, Dissociation, and Psychosis: CBT and Other Approaches to Understanding and Recovery - An Online Course
Free Offer: Presentation on “Understanding Psychosis as an Attempt to Solve Problems: Integrating Perspectives on Trauma, Spirituality and Creativity”
Click the link below to access this recording that explores some of the trickiest aspects of "psychosis," and also to receive notices periodically about online courses and webinars that may become available.
http://eepurl.com/cMAgI
Old belief systems die slowly. SSRI’s clearly induce mania in a subset of people. A general activation that can range from mood elevation to Psychosis to Akathisia. But psychiatrists were trained that means they have “underlying bipolar disorder”. Evidence to support this.. hell
I thought for a second: “if you wanted to create mass confusion and mental anguish in a generation what would you do?” Well… you would condition them to think that every aversive emotion or thought has nothing to do with a valid reaction to events in their life, get them to
"Growing up, I was sold the idea that the only way to get people to take your mental struggles seriously is to call them illness. Paradoxically, it was only when I abandoned this idea that I reached a deeper appreciation of the seriousness of my suffering..."
Another taboo topic: do ‘antipsychotics’ cause withdrawal symptoms? @joannamoncrieff @markhoro @CEP_UK @MarnieWedlake @dranneguy @IndigoDaya @Institute_PDW
I’m honored to be giving a talk organized by ISPS Poland tomorrow on the topic: Recovery A Conspiracy of Hope. It's free to join and will stream at 8pm Central European Time.