I’ve been intrigued by the way the battle against mental health system oppression has drawn on two important and powerful ideas – which happen to contradict each other!
One is the idea that people can “recover” from mental health problems. Asserting the possibility of recovery has been key to fighting back against the oppressive belief that certain people will always be “mentally ill” and will need to resign themselves to a limited life as a mental patient, etc.
The second idea is that people may not have to change to be OK and valuable – that people can even be proud of what has been called madness! Mad pride helps people fight back against the oppressive notion that one has to be “normal” to be acceptable, and that mental diversity means illness.
But, if one is perfectly OK as one is, then there is no need for recovery. In fact, if one is already quite OK, then the suggestion that one should work on recovery can itself be oppressive – like offering “reparative therapy” for gay people.
On the other hand, if one’s mental state and current beliefs are causing lots of problems that are keeping one stuck, then being encouraged to be proud of that mental state can become a barrier to changing or recovering and so can deepen or prolong problems and oppression.
Contradictions like those outlined above can lead to battles between activists about how to move forward. They can also lead to battles, and confusion, within people who are trying to find the best way to deal with their own “mad” states.
What I want to show is that it’s possible to embrace both “recovery” and “mad pride” despite the contradictions. But to do so, we need to be aware of both the advantages, and of the “down” or “shadow” side of each of these notions.
Let’s start by looking at the concept of recovery.
Compared to mad pride, recovery has been much more widely embraced. It has even been embraced by much or most of the mental health system – though often what is embraced is just the word itself, and not the possible reality! But because of its popularity, it has also been more widely critiqued, and some have even advocated that we stop using the word altogether.
One common critique is that the word “recovery” implies that one must have been ill in the first place, and so this word should not be used when the problem never was an “illness.” However, people do “recover” from many things that aren’t an illness: we recover our balance, we recover from injuries, we even recover from the down side of events that were overall positive, as in “I’ve finally recovered from that wild party I attended last night!” Krista Mackinnon, in her “Recovering Our Families” course, emphasizes that all humans are constantly recovering from all sorts of things, and so “recovery” is not something unique to those who have been psychiatrically labeled.
A stronger critique of the notion of recovery points out that recovery involves going back to something, while many prefer to see their life as going forward. John Herold for example talks about wanting to move toward “discovery” and not “recovery.” I agree with that up to a point, but I also notice that we often have to go back to something we had possessed previously in order to move forward overall. For example, if I used to know how to face people and maintain friendships, but then I seemed to have lost that ability during an emotional crisis, I may want to recover the skills and habits I had before so that I can then get on with my life and move into that wider process of discovery.
Then there’s the problem of the word being co-opted to mean something much less than real recovery. Lots of mental health programs use the recovery word, but their practices remain targeted towards lifelong drugging and containment of the person, with “recovery” apparently meaning only getting to where the person won’t be in crisis so much. I understand why that sort of use of the word “recovery” makes people want to vomit, but I would rather work on reclaiming the word, rather than giving it up. The US government can call a nuclear missile a “Peacekeeper” but that doesn’t mean we need to quit using the word “peace.” I think our best strategy is to continue to emphasize the true meaning of recovery and to contrast truly recovery-oriented treatment with that which is not.
Adding complexity to discussions of recovery is the distinction between “clinical recovery,” or no longer experiencing “symptoms,” versus “personal recovery” which has been defined as “recovering a life worth living.”
Interestingly, within standard care, “personal recovery” is often framed as the proper goal because of a belief that “clinical recovery” is not possible. In other words, it is believed that the person will always have symptoms and will always be less than healthy than others because of that, but they may still learn to “recover a life worth living” despite continuing to be ill. (Of course, this notion that they are still ill can be used to convince people to stay on their drugs, which makes this interpretation popular amongst those who embrace the medical model but who still want to offer some appearance of hope.)
But there is a deeper and more valid reason to focus on personal recovery rather than clinical. That’s because the experiences that the mental health system called “symptoms” may not be a problem at all once the person learns to live with them. Hearing voices for example may be benign or even helpful once the person learns to relate to them differently. And once experiences no longer cause problems, there is no longer a need for drugs or any kind of treatment to manage them.
Of course, it’s the idea that people don’t need to change, and that their differences may be OK or even something quite valuable, that is basic to that idea that sometimes seems in opposition to recovery: mad pride.
“You are only given a little spark of madness. You mustn’t lose it.” Robin Williams
From a radical mad pride perspective, there is only mental diversity, and not any mental problems, disorders, or illnesses. People do best when they accept and become proud of themselves as they are rather than try to change. If people have problems, or seem to be disabled in some way, it’s just because society has failed to accommodate their differences, and so it’s society that needs to change.
But what are the problems with this kind of radical mad pride perspective?
One issue is that if I am suffering in some way, while believing that there is nothing wrong with me but only problems with others, and if it’s also true that I don’t have the power to make others change, then I am stuck with my suffering. Working on recovery from a problem may not require accepting that one is ill, but it at least requires accepting that something needs to be changed; but pride is the opposite of believing in a need for change.
Another problem is the adversarial relationships that a radical mad pride perspective can create with others. If I for example demand that others change their attitudes and start accepting me just as I am and if I demand that they change in other ways to accommodate my differentness, while I insist that I am perfectly fine as I am and don’t need to change anything, I may just piss people off. I’m certainly not likely to be effective at winning friends and forming peaceful relationships, since good relationships tend to be built when people are willing to change at least some to accommodate each other, at least when they are able to do so.
On the other hand, the notion of radically accepting ourselves just as we are can often seem to be the very core of peace of mind and mental healing. So it can all seem quite complex.
How can all this be best resolved? Or, how can we take what is best about mad pride, and what is best about recovery, without getting caught up in the shadow side of each?
I think it may help to take a step back, and look in more general terms at how we can resolve other kinds of contradictions.
It’s not uncommon that things are opposites, but we find ourselves needing both. Breathing in for example is a good thing, but so is breathing out, even though that’s the opposite. Our ability to open up to people and trust is a good thing, but so at certain times is our ability to close up and distrust.
Mental health issues can be notoriously complex. People can go through terrifying, bewildering experiences that may also have a very important positive side. Or, experiences may seem to be quite positive, but then lead to something very detrimental.
It’s also possible that an experience we want to recover from at one point may be something that later we wish to regain. In my own life I can identify times I have worked to recover from “madness” and to regain my ability to integrate with normality, and then also times when it seemed more important to turn around and work to recover from that normality trance, so I could reclaim what I had discovered when I first went “out of my mind.”
One metaphor for madness is that of revolution. Revolution overthrows the existing order – then anything is possible, which is both great, and terrible. Revolution is both something to be proud of, when it is necessary and when it works out well, and it is something to recover from, so that order can be restored.
When we over-value sanity, we stick with an existing order in rigid ways that can be oppressive. When we over-value madness, or revolts against sanity, we can get lost in disorder. Life though works best at the edge of chaos and order, so it may require both rebellion against order and efforts to recover order.
One way to map relations between polarities, where neither polar opposite provides a full answer, is to use what is called a polarity management map. These maps make overt what is positive and negative about each polarity, and suggest that each polarity is the solution for the problems caused by the other.
Below is a polarity management map about recovery versus mad pride. It suggests that there is no final answer to resolving the tensions between mad pride and recovery, or between madness and sanity generally. Rather, whenever we emphasize the positive of one side, we will also sooner or later encounter its negative, and then may have to shift to the opposite side.
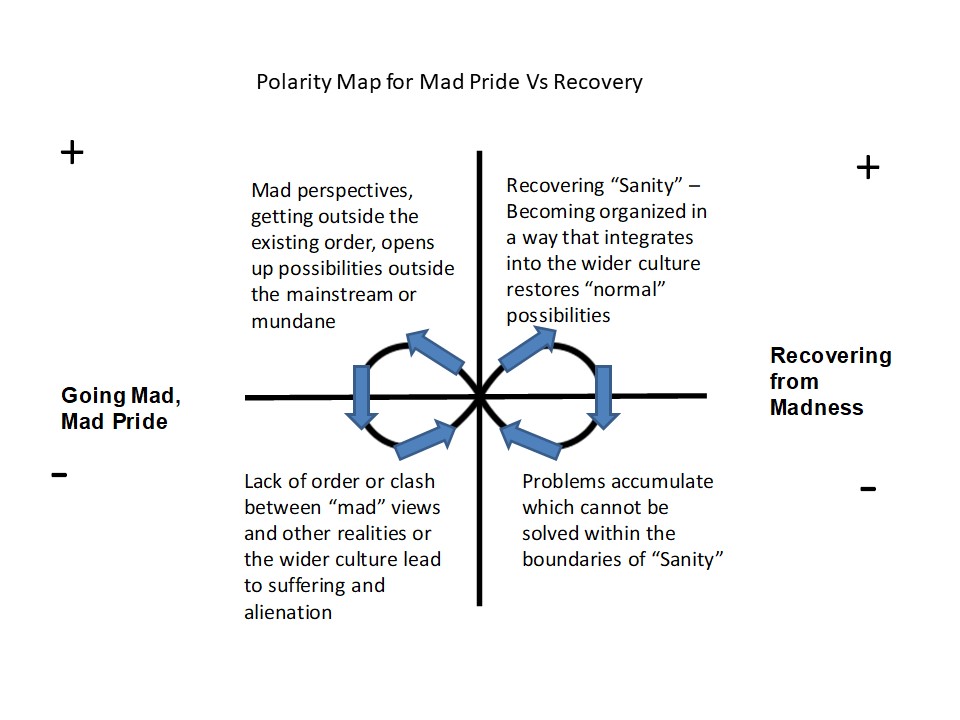
If we follow this line of thinking, it follows that there are no final answers as to when a focus on change and recovery is best, versus when it might be better to instead be proud of one’s current state and perspective, even if it is somewhat “mad.” Instead, we will be more open to exploring what might fit or seem healthy, or not, in any given situation. And we will be open to the possibility that whatever we choose now, we will later be called upon to choose the opposite.
When we are too sure that our side is right, that “God is on our side,” we end up at war with our opposite. People who are too sure that their current mental view or version of sanity is correct will go to war against that which opposes it, be they voices or other people who are seen mentally wrong But going to war just makes everything more extreme, and prevents the “peaceful revolutions” that are possible when people realize that their current polarity is just one side of a more complex picture.
Modern humans are not, of course, the first to struggle with these issues. Spiritual traditions going back to ancient times wrestle with how to relate to the limits of any existing order, and how to find value in what is outside of that order, or “outside of our minds.” While these traditions are not perfect, and have too many times been bent to completely corrupt and oppressive purposes, they also contain reminders that we humans do our best not when we stay confined within a mundane “sanity” but rather when we allow ourselves, at least at times, to open up to what goes beyond.
What would mental health treatment look like if it balanced an awareness of the need for “recovery” with an awareness that people also sometimes need to go “out of their minds” to resolve problems that they haven’t been able to solve otherwise, or maybe that their entire culture has not been able to face and resolve?
To explore some possible answers to that question, I recently put together a new online course, “Addressing Spiritual Issues Within Treatment for Psychosis and Bipolar.” This course outlines some radically different ways of conceptualizing the mental states that get called “psychosis” and “bipolar” and reviews ways professionals can shift from pretending to “know it all” to being helpful to people as they face some of the bigger mysteries together. In the course, I try to strike a balanced position that avoids both “romanticizing” extreme states and the more common mistake of “awfulizing” or “pathologizing” them.
This course comes with 6 CE for most US professionals. Use this link to get more information, or to register.
A few more thoughts:
One other possibly helpful metaphor for madness is that of wilderness.
It can be disturbing when young people wander off into the wilderness. What if they become lost, and need to be rescued? Sometimes people do need to be rescued. But a society too sure that the wilderness is nothing but bad will seek to prevent young people from ever wandering off, won’t recognize when people are doing OK in their explorations and don’t need to be rescued, and/or will even seek to destroy the wilderness so that everything can be “civilized” – aka, sane.
But any society cuts itself off from the wilderness, and/or declares war on what is wild, only at its own peril. Certainly, modern civilization or “normality” has declared war on the wild, and it does often seem that it is winning. But that “winning” is a most terrible thing, and puts us all in danger!
Rather than winning, we need to focus more on finding a dynamic balance, or peaceful coexistence. The peaceful coexistence between recovery and mad pride that I have proposed is just one example of that.
Emerson said that “People wish to be settled; only as far as they are unsettled is there any hope for them.” It’s time that we define mental health not as some settled “sanity” but as the unsettled and possibly playful dialogue that results when we value both madness and sanity, and when we explore together with those whom we wish to help rather than impose our own version of some settled, and dead, “correct answer.”


